
A Fully Functional Drug-Eluting Joint Implant
Suhardi, VJ, et. al. Nature Biomedical Engineering. 2017;1
Summary
Research Focus: To improve prosthetic joint infection (PJI) revisions of the hip and knee. The current procedure for such PJI revisions is a two-step, long-term protocol that can be complicated by joint dislocations, fractures and/or bacterial infections. The authors here aimed to develop and to test a one-step surgery, where the replacement, drug-eluting joint material can both resolve local infection challenges and provide adequate, mechanical strength for safe, long-term use.
Scientific Contributions of the Publication: An innovative, single-stage protocol for the resolution of knee and hip PJIs was developed, tested and found to be significantly better than the current clinical gold standard of care, both in terms of resolving local bacterial challenges, and in its overall mechanical performance.
Optical Imaging Data
Clearance of Planktonic S. aureus challenge in PJI Model: Tested New Antibiotic-Joint Material Blend vs. Current Gold Standard Bone Cement Blend
A commonly used antibiotic drug eluting Bone Cement (BC) spacer formulation, and an optimized vancomycin-Ultra High Molecular Weight Polyethylene (UHMWPE) blend were evaluated for their relative efficacies against planktonic S. aureus challenges:
Animal Model: Male, 12 month-old, fully immune-competent, skeletally mature New Zealand rabbits.
Dual, Planktonic Bacterial Challenges:
-
5 x107 CFU/mL aureus (Xen29, from PE) in 50uL 0.9% saline, intra-tibial canal, and
-
5 x107 CFU/mL S. aureus (Xen29, from PE) in 50uL 0.9% saline, intra-articular (Figure 2)
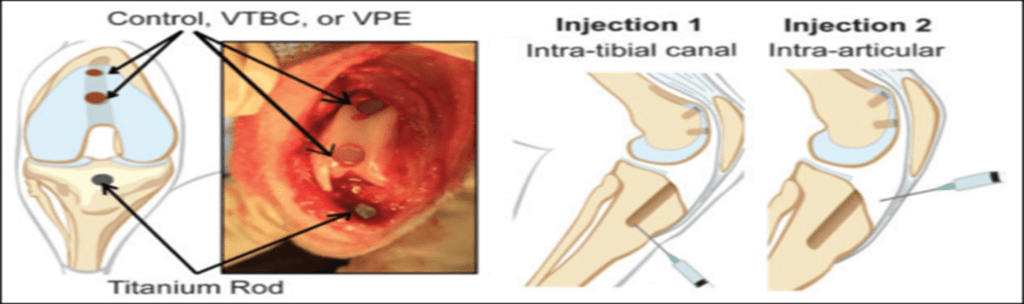
Figure 1. Locations of dual, planktonic, bioluminescent S. aureus (Xen 29) challenges (intra-tibial and intra-articular), titanium rod plug, and dual treatment plugs of: control, VTBC, or VPE, n = 5/treatment group.
No additional antibiotics were provided to the test rabbits over the course of the efficacy study. At 3-weeks post bacterial challenge, an in situ bioluminescent imaging analysis was done to determine relative S. aureus load in the treatment groups.
Treatment Groups (n=5/group, Figure 1):
-
Control: No antibiotic material in UHMWPE
-
VTBC: 2.3 wt% vancomycin HCl, 8.3 wt% tobramycin in Bone Cement, and
-
VPE: 7.0 wt% vancomycin HCl in ULMWPE
End Point Observations:
-
Survival at 21-days post challenge: Controls = 0%; VTBC = 40%, and VPE = 60% (see Figure 3a).
-
No BLI signal detected in any of the VPE-treated rabbit knee joints, while total bioluminescent flux in both VTBC and control groups were significantly greater (Student’s t-test, *p <0.05, see Figure 2b, c).
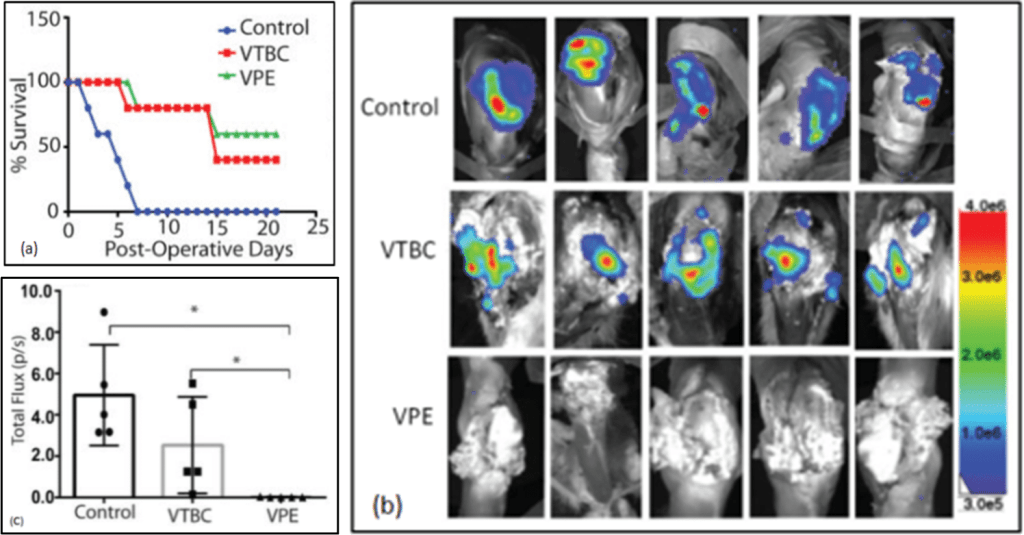
Figure 2. For control, VTBC and VPE treatment groups: Survival graph over study time course (a), S. aureus in situ bioluminescent signal in rabbit knee joints at 21-days post challenge (b), and total bioluminescent total flux data, mean +/- SD, *p <0.05 (c). For additional results supporting this optical data, see publication.
Clearance of S. aureus biofilm challenge in PJI Model: New Rifampin-Vancomycin-UHMWPE blend vs. Current Gold Standard BC
Biofilms at the bone-implant interface are difficult to treat due to limited penetration of systemically administered antibiotics. The current state-of-the-art antibiotic regimen against G+/G- biofilms is to use a synergistic combination of rifampin and vancomycin. Rifampin-vancomycin (rif-vanco) synergy can reduce bacterial vancomycin MIC, and prevent rapid rifampin resistance, as is seen when rifampin is used alone.
Following clinical guidelines for an optimal rif-vanco synergy, authors selected a rif:vanco mass ratio of 1:2.5, respectively, and after considering required mechanical Ultimate Tensile Strength and Impact Strength values (see publication), they went with a 3.3 wt% rifampin and 6.7 wt% vancomycin in an UHMWPE blend.
Animal Model: Male, 12 month-old, fully immune-competent, skeletally mature New Zealand rabbits.
Biofilm Bacterial Challenge:
All rabbits received a beaded titanium rod covered with a fully grown bioluminescent S. aureus (Xen 29) biofilm, in the tibial canal (Figure 3a). Note that there was no significant difference the bacterial load between treatment groups (Figure 3b).
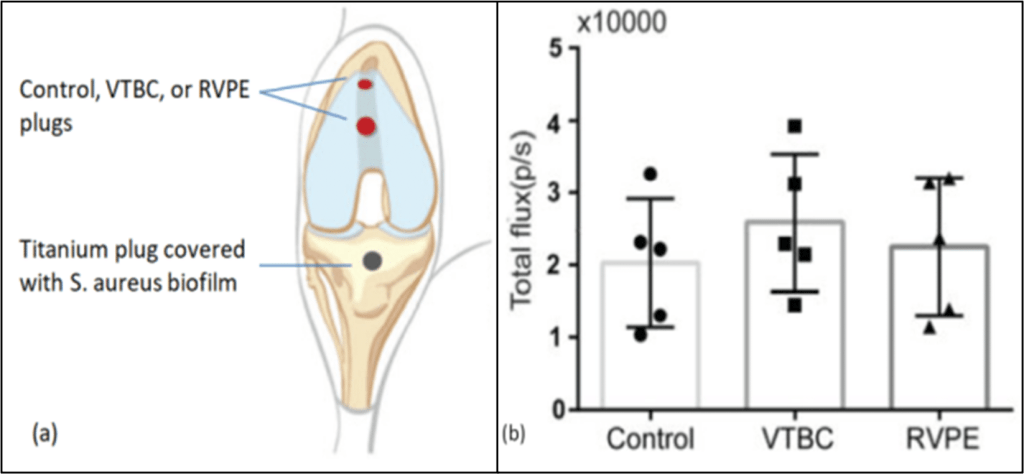
Figure 3. Locations of titanium plug covered with bioluminescent S. aureus (Xen 29) biofilm, and dual treatment plugs of control, VTBC, or RVPE; n = 5 per treatment group (a), S. aureus biofilm total bioluminescence flux per titanium rod, p/s, mean +/- SD (b).
Treatment Groups (n=5/group, Figure 4):
-
Each rabbit received two treatment plugs in the patellofemoral groove, where treatments were:
-
Control: No antibiotic material in UHMWPE
-
VTBC: 2.3 wt% vancomycin HCl, 8.3 wt% tobramycin in Bone Cement, and
-
RVPE: 6.7 wt% vancomycin HCl, 3.3 wt% rifampin in ULMWPE
No additional antibiotics were given to test rabbits over the efficacy study time course. At 3-weeks post challenge, relative S. aureus loads in the treatment groups were evaluated by in situ bioluminescent imaging.
End Point Observations:
-
Survival at 21-days post challenge: Controls = 0%; VTBC = 20%, and RVPE = 100% (Figure 4a).
-
No BLI signal detected in any of the RVPE-treated rabbit knee joints, while total bioluminescent flux in both VTBC and control groups were significantly greater (Student’s t-test, *p <0.001, Figure 4b, c).
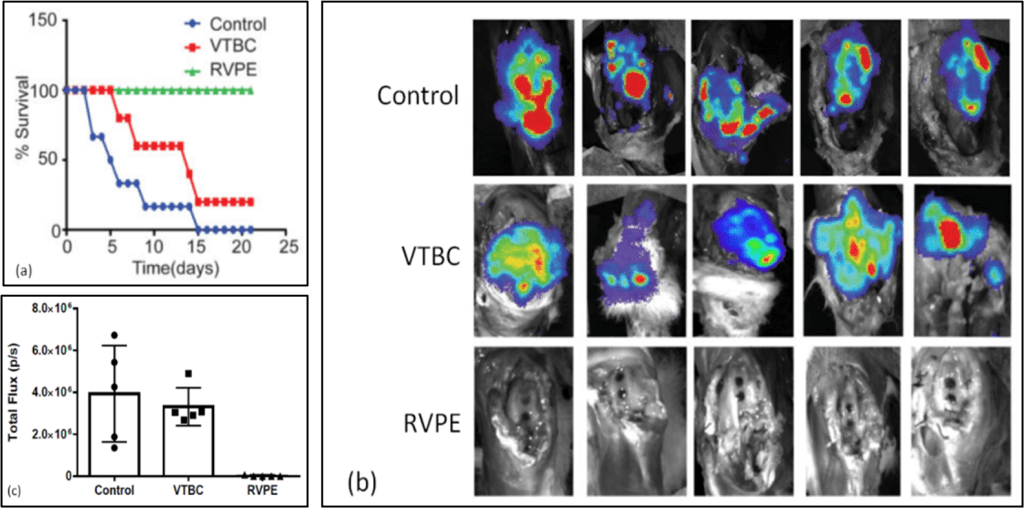
Figure 4. For control, VTBC and RVPE treatment groups: Survival graph over study time course (a), S. aureus in situ bioluminescent signal in rabbit knee joints at 21-days post challenge (b), and total bioluminescent total flux data, mean +/- SD, *p <0.001, (c) . For additional results supporting this optical data, see publication.

